Guidelines
Patients who may be appropriate for Zypitamag® (pitavastatin)
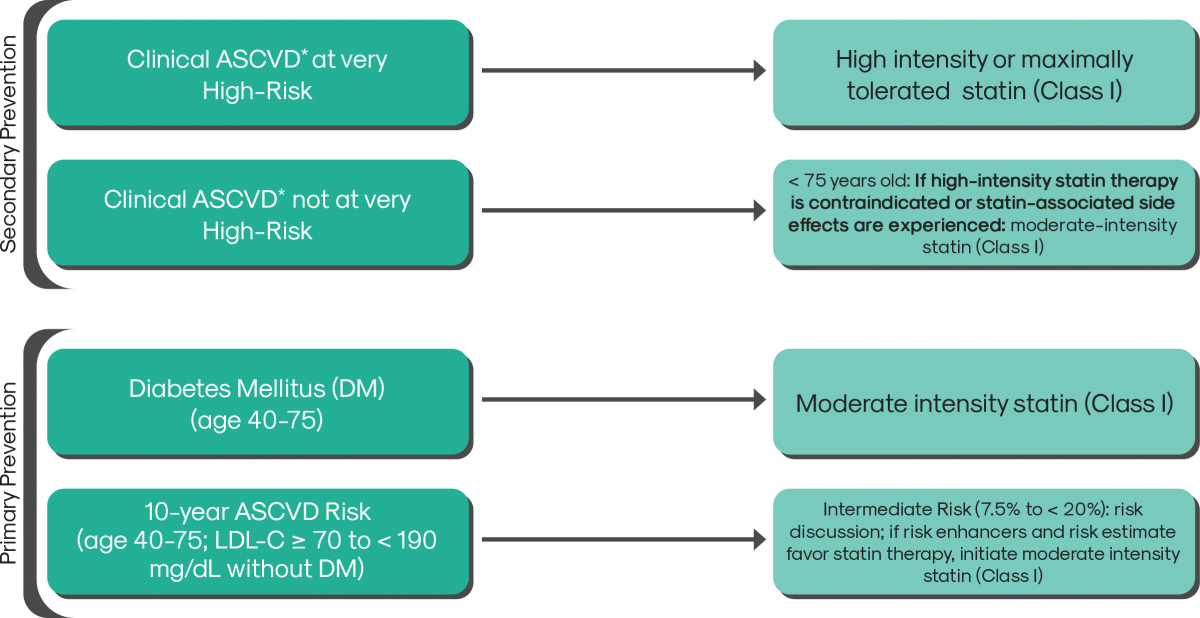
As per the new 2018 ACC/AHA Multisociety Guidelines on the Management of Blood Cholesterol, all doses of Zypitamag are now considered Moderate Intensity
* ASCVD (atherosclerotic cardiovascular disease) consists of ACS (acute coronary syndrome), those with history of MI (myocardial infarction), stable or unstable angina or coronary other arterial revascularization, stroke, transient ischemic attack (TIA), or peripheral artery disease (PAD) including aortic aneurysm, all of atherosclerotic origin.
Very high-risk includes a history of multiple major ASCVD events or 1 major ASCVD event and multiple high-risk conditions.
Individual responses to statin therapy varied in the RCTs and should be expected to vary in clinical practice.
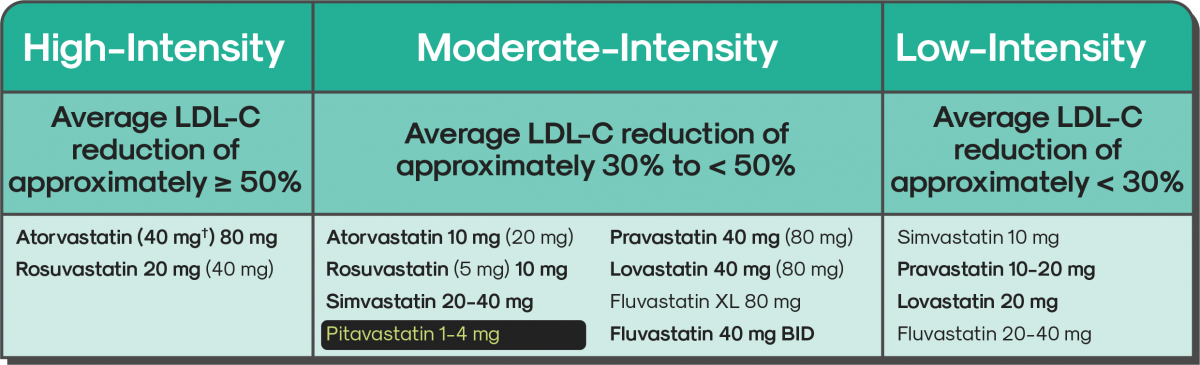
† Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in the IDEAL (Incremental Decrease through Aggressive Lipid Lowering) study.
Percent LDL-C reductions with the primary statin medications used in clinical practice (atorvastatin, rosuvastatin, simvastatin) were estimated using the median reduction in LDL-C from the VOYAGER database. Reductions in LDL-C for other statin medications (fluvastatin, lovastatin, pitavastatin, pravastatin) were identified according to FDA-approved product labeling in adults with hyperlipidemia, primary hypercholesterolemia, and mixed dyslipidemia.
Boldface type indicates specific statins and doses that were evaluated in RCTs, and the Cholesterol Treatment Trialists' 2010 meta-analysis. All of these RCTs demonstrated a reduction in major cardiovascular events.
BID indicates twice daily; FDA, U.S. Food and Drug Administration; LDL-C, low-density lipoprotein cholesterol; RCT, randomized controlled trial; VOYAGER, an indiVidual patient data meta-analysis Of statin therapY in At risk Groups: Effects of Rosuvastatin, atorvastatin and simvastatin; and XL, extended release.
References:
Grundy et al. J Am Coll Cardiol 2018;Nov 10:[Epub ahead of print]
IMPORTANT SAFETY INFORMATION FOR ZYPITAMAG™ (pitavastatin) tablets
INDICATIONS & USAGE
ZYPITAMAG is indicated as an adjunct to diet to reduce low-density lipoprotein cholesterol (LDL-C) in adult patients with primary hyperlipidemia.
Pediatric use information is approved for Kowa Co Ltd LIVALO (pitavastatin) tablets. However, due to Kowa Co Ltd marketing exclusivity rights, this drug product is not labeled with that information.
CONTRAINDICATIONS
ZYPITAMAG is contraindicated in the following conditions:
- Concomitant use of cyclosporine.
- Acute liver failure or decompensated cirrhosis.
- Hypersensitivity to pitavastatin or any excipients in ZYPITAMAG. Hypersensitivity reactions including angioedema, rash, pruritus, and urticaria have been reported with pitavastatin.
WARNINGS & PRECAUTIONS
- Myopathy and Rhabdomyolysis: Risk factors include age 65 years or greater, uncontrolled hypothyroidism, renal impairment, concomitant use with certain other drugs (including other lipid-lowering therapies), and higher ZYPITAMAG dosage. ZYPITAMAG is contraindicated in patients taking cyclosporine and not recommended in patients taking gemfibrozil. The following drugs when used concomitantly with ZYPITAMAG may also increase the risk of myopathy and rhabdomyolysis: lipid-modifying dosages of niacin (>1 g/day), fibrates, and colchicine. Discontinue ZYPITAMAG if markedly elevated CK levels occur or if myopathy is either diagnosed or suspected. Temporarily discontinue ZYPITAMAG in patients experiencing an acute or serious condition at high risk of developing renal failure secondary to rhabdomyolysis; e.g., sepsis; shock; severe hypovolemia; major surgery; trauma; severe metabolic, endocrine, or electrolyte disorders; or uncontrolled epilepsy. Inform patients of the risk of myopathy and rhabdomyolysis when starting or increasing the ZYPITAMAG dosage. Instruct patients to promptly report any unexplained muscle pain, tenderness or weakness particularly if accompanied by malaise or fever.
- Immune-Mediated Necrotizing Myopathy (IMNM): There have been rare reports of IMNM, an autoimmune myopathy, associated with statin use, including reports of recurrence when the same or a different statin was administered. IMNM is characterized by proximal muscle weakness and elevated serum creatine kinase that persist despite discontinuation of statin treatment; positive anti-HMG CoA reductase antibody; muscle biopsy showing necrotizing myopathy; and improvement with immunosuppressive agents. Additional neuromuscular and serologic testing may be necessary. Treatment with immunosuppressive agents may be required. Discontinue ZYPITAMAG if IMNM is suspected.
- Hepatic Dysfunction: Increases in serum transaminases can occur. Rare postmarketing reports of fatal and non-fatal hepatic failure have occurred. Consider liver enzyme testing before initiating therapy and as clinically indicated thereafter. If serious hepatic injury with clinical symptoms and/or hyperbilirubinemia or jaundice occurs, promptly discontinue ZYPITAMAG.
- Increases in HbA1c and Fasting Serum Glucose Levels: Increases of each have been reported with statins, including ZYPITAMAG. Optimize lifestyle measures, including regular exercise, maintaining a healthy body weight, and making healthy food choices.
ADVERSE REACTIONS: The most frequent adverse reactions (rate ≥ 2%) are myalgia, constipation, diarrhea, back pain, and pain in extremity. This is not a complete list of all reported adverse events.
For additional information, refer to full Prescribing Information.
You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.FDA.gov/medwatch or call 1-800-FDA-1088.
